Mobile Health’s Growing Pains
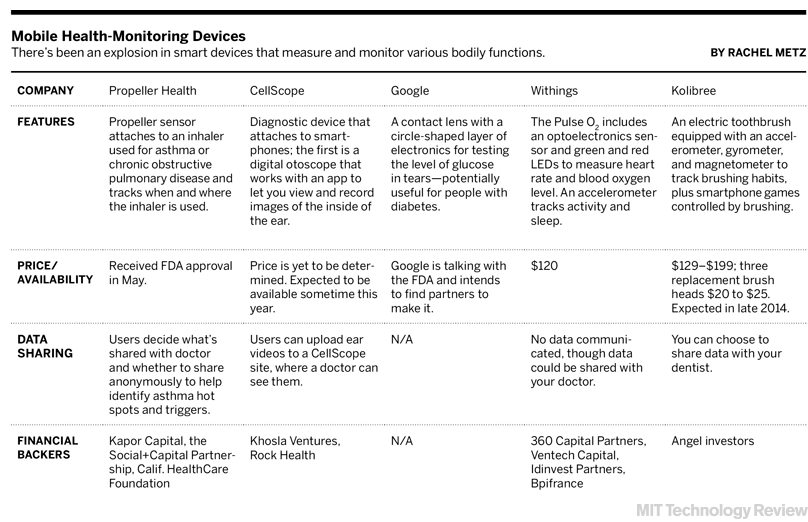
Among technologists, mobile health is thriving. Since the start of 2013, more than $750 million in venture capital has been invested in companies that do everything from turn your smartphone into a blood pressure gauge to snapping medical–quality images of the inner ear. Apple, Qualcomm, Microsoft, and other corporate giants are creating mobile health products and investing in startups.
The idea is straightforward: the increasing number of smartphones means that small, inexpensive sensors, low-energy Bluetooth, and analytic software make it possible for patients and doctors to capture all kinds of data to improve care. Patients can play a more active role in their own health. Doctors and nurses can make house calls without ever leaving the office.
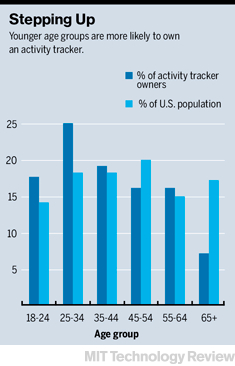
One crucial group, however, remains unsold: the patients. Though one in 10 Americans owns the type of tracking device made by Nike, Fitbit, and Jawbone to monitor steps taken, quality of sleep, or calorie intake, more than half of those devices are no longer in use, according to Endeavour Partners, a consulting firm. Of the 100,000-plus mobile health applications available for smartphones, very few have been downloaded even 500 times. More than two-thirds of people who downloaded one have stopped using it, according to a 2012 study done for the global accounting firm PWC.
“There are unrealistic expectations for when and how mobile health is going to come together,” says Patty Mechael, former executive director of the mHealth Alliance, which helped develop early standards for mobile health technologies. In the U.S. “we are somewhere between the peak of the hype cycle and the trough of disillusionment,” she says.
Enthusiasm has been slow to build in part because the technology is often still not perfect, with seemingly simple functions like step counters lacking precision. Another problem is motivation. Many people simply don’t seem to like using these apps and devices. It is clear, though, that a well-designed mobile health system can help if patients use it.
At the Center for Connected Health at Partners HealthCare, a health-care network that includes Boston’s two leading hospitals, Brigham and Women’s and Massachusetts General, a number of mobile programs have been shown to offer strong payoffs both in quality and cost.
One recent study tested whether mobile phones could help increase activity among patients with diabetes. It’s an important way to combat the disease’s progression, but it’s something traditional programs have had little success achieving. Of a group of 130 patients with diabetes, half were given Fitbit activity monitors. By combining feedback from the Fitbit with existing patient records, an algorithm determined which text messages would be sent to the patients. Those falling behind on their goals got messages of encouragement; some messages included information about nearby Zumba classes or jogging paths, based on location data picked up from the patients’ mobile devices. On rainy days, the program might send a note about ways to exercise indoors.
Doctors received progress updates via a stoplight system displayed on the patient’s electronic medical record. Green meant the patient was doing well. Yellow was caution. Red signaled the patient was not responding to the text messages.
After six months, the average patient was walking about a mile farther each day. In addition, the patients’ blood sugar control improved significantly—better results than might be expected with some FDA-approved drugs, says Kamal Jethwani, a doctor who ran the study as the center’s leader of research and program evaluation.
For Partners, the program is successful on two counts: patients are healthier, and the cost of caring for them is lower. The payoff for better managing a chronic disease like diabetes comes over many years, but in Jethwani’s study, a number of patients have already had drops in blood sugar that equate to savings of $1,000 to $1,200 in doctor visits and other treatments. That’s a strong return on a program that costs $300 per patient to run, notes Jethwani.
-->
These are the kinds of results that have enthusiasts convinced that mobile technology can not only fundamentally overhaul how health care is delivered, but also offer sufficient financial benefit to convince insurers and patients to pay for it.
John M. Halamka, a professor at Harvard Medical School and chief information officer of Beth Israel Deaconess Medical Center, expects this kind of technology-enabled monitoring to become standard practice within the next few years. One sign that a heart patient may be about to have a problem is rapid weight gain, he notes. A smart scale that picks up on that could trigger a quick intervention from the doctor and avoid a visit to the ER.
At the University of California, San Francisco, which recently announced an initiative to begin testing the effectiveness of mobile devices in health care, one of the biggest technological achievements to date was simply starting to get doctors to move beyond pagers. Now doctors access patient messages via a mobile or Web application, and the message automatically becomes part of a conversation. Under the new system, the whole care team is aware of what is happening, and the doctor has the patient’s history available when fielding questions. A program is being tested that would take this to the next level, allowing care providers to send messages to patients.
Getting mobile health technology right can be tricky, however. Fitbit makes some of the most popular activity trackers, but in February the company voluntarily recalled its top-of-the-line $129 Fitbit Force after users complained of skin irritation from the wristband. More serious technological problems have sidelined devices aimed at difficult tasks like measuring blood glucose levels without drawing blood, a desirable feature for people with diabetes.
For all the challenges in mobile health, one issue that dominates many discussions about the technology may fade rather quickly. Privacy concerns have yet to come up in the Partners trial, says Jethwani. “I’ve never heard any patient say, ‘How do you know so much about me?’ or ‘Why do you know so much?’” he says. “Instead, they say ‘Now that you know all this about me, can you give me more useful information?’”
Keep Reading
Most Popular
Large language models can do jaw-dropping things. But nobody knows exactly why.
And that's a problem. Figuring it out is one of the biggest scientific puzzles of our time and a crucial step towards controlling more powerful future models.
The problem with plug-in hybrids? Their drivers.
Plug-in hybrids are often sold as a transition to EVs, but new data from Europe shows we’re still underestimating the emissions they produce.
Google DeepMind’s new generative model makes Super Mario–like games from scratch
Genie learns how to control games by watching hours and hours of video. It could help train next-gen robots too.
How scientists traced a mysterious covid case back to six toilets
When wastewater surveillance turns into a hunt for a single infected individual, the ethics get tricky.
Stay connected
Get the latest updates from
MIT Technology Review
Discover special offers, top stories, upcoming events, and more.